Two people can look nearly identical in a mirror and have completely different health profiles. One carries most of their fat just under the skin — soft, visible, pinchable. The other carries theirs packed around their internal organs — invisible from the outside, metabolically active, and associated with significantly higher health risk. The number on the scale treats both the same. So does BMI. So does your bathroom mirror.
Subcutaneous fat and visceral fat are not just two names for the same thing. They behave differently, respond to different interventions, carry different health implications, and require different tools to measure. Here's the honest breakdown of each.
Visceral Fat vs Subcutaneous Fat: The Key Differences
| Property | Subcutaneous Fat | Visceral Fat |
|---|---|---|
| Location | Directly under the skin — belly, hips, thighs, arms | Deep inside the abdominal cavity, surrounding the liver, intestines, and other organs |
| Can you see it? | Yes — it's the visible belly, love handles, and soft areas you can pinch | No — entirely hidden beneath the abdominal muscles |
| Can you pinch it? | Yes — caliper measurements work on subcutaneous fat | No — calipers cannot reach visceral fat |
| Health risk profile | Lower risk at moderate levels; associated with cosmetic concerns more than metabolic disease | Higher risk — strongly linked to insulin resistance, type 2 diabetes, cardiovascular disease, metabolic syndrome |
| How to measure it | Calipers, visual assessment, DEXA scan, body fat % | CT scan or MRI (accurate); waist circumference (proxy); DEXA (estimated) |
| How quickly it changes | Slower to mobilize, especially from hips and thighs | Responds faster to diet and exercise intervention than subcutaneous fat |
| Visible in progress photos? | Yes — subcutaneous reduction shows up in the mirror and in photos | No — visceral fat reduction is invisible in photos even as health improves dramatically |
What Is Subcutaneous Fat?
Subcutaneous fat is the fat stored directly beneath the skin — the soft tissue you can grab with your fingers. It sits between the skin and the underlying muscle layer and is distributed across the entire body: abdomen, hips, thighs, arms, and back. When you look in the mirror and see a belly, love handles, or soft spots on your arms, you're seeing subcutaneous fat.
Subcutaneous fat serves real physiological functions. It insulates the body, cushions against impact, stores energy, and plays a role in hormone production. Some amount is not only normal but necessary. The health risks associated with subcutaneous fat at moderate levels are relatively limited compared to visceral fat — though very high levels of subcutaneous fat are still associated with elevated cardiometabolic risk.
Subcutaneous fat also shows significant individual and sex-based distribution patterns. Women tend to store more subcutaneous fat in the hips, glutes, and thighs (a "pear" distribution). Men tend toward the abdomen. These patterns are hormonally influenced — estrogen directs fat toward peripheral storage, testosterone toward abdominal storage. This is part of why the same total body fat percentage looks different on different people.
What Is Visceral Fat?
Visceral fat is stored inside the abdominal cavity — wrapped around the liver, intestines, stomach, and other internal organs. It sits behind the abdominal muscles, invisible from any external view. You cannot see it, pinch it, or feel it directly. A person can have a relatively flat stomach and still carry dangerous amounts of visceral fat. A person can have a noticeable belly composed almost entirely of subcutaneous fat with minimal visceral accumulation.
Unlike subcutaneous fat, visceral fat is highly metabolically active. It secretes inflammatory cytokines and adipokines — signaling molecules that influence insulin sensitivity, inflammation, and cardiovascular function. This is why elevated visceral fat is so strongly associated with metabolic syndrome, type 2 diabetes, non-alcoholic fatty liver disease, and cardiovascular disease. The fat you can't see carries more metabolic consequence than the fat you can.
How to Tell Which Type You Carry More Of
Without imaging (CT or MRI), you cannot measure visceral fat directly. But several indirect signals give you a reasonable estimate:
| Signal | What It Suggests | Limitation |
|---|---|---|
| Waist circumference | Over 40 inches (men) / 35 inches (women) is associated with elevated visceral fat risk | Doesn't distinguish visceral from subcutaneous — just total abdominal volume |
| Waist-to-hip ratio | Apple shape (waist > hips) correlates more with visceral fat than pear shape | Still indirect; influenced by subcutaneous distribution |
| Belly texture | Soft, pinchable belly → more subcutaneous. Hard, distended belly that doesn't compress → more visceral | Subjective; requires palpation experience |
| DEXA scan | Provides android fat mass estimate that correlates with visceral fat | Can't isolate visceral from subcutaneous abdominal fat directly |
| CT / MRI scan | Directly images visceral fat volume — research gold standard | Expensive, requires medical access, not for routine tracking |
For most people, waist circumference is the most practical proxy. Research consistently shows that waist circumference above the thresholds above is associated with elevated visceral adiposity and increased metabolic risk, independent of total body weight or BMI.
What Progress Photos Can and Can't Tell You
This is the honest limitation that most body composition content avoids saying directly: progress photos — including AI body composition analysis — track subcutaneous fat, not visceral fat. The camera sees the surface. It cannot image what's happening behind your abdominal wall.
This means a few things in practice:
First, visible progress in photos is real progress — subcutaneous fat reduction improving your appearance is meaningful. Losing subcutaneous belly fat is a genuine health win and reflects an overall reduction in energy balance that very likely also reduces visceral fat simultaneously.
Second, the absence of visible progress does not mean visceral fat isn't changing. Visceral fat often responds faster to caloric deficit and exercise than subcutaneous fat does. A person two weeks into a fat loss phase might have already reduced their visceral fat load meaningfully while their mirror still looks identical.
Third, a lean-looking person can still carry elevated visceral fat — particularly someone who is "skinny fat": low muscle mass, moderate body fat, but a disproportionate visceral fat burden due to sedentary lifestyle. Progress photos would show them as lean. Metabolically, the picture is more complex.
How to Reduce Both
The good news: the interventions that reduce visceral fat and subcutaneous fat overlap almost entirely. You don't need a separate protocol for each. A caloric deficit combined with resistance training and aerobic exercise addresses both. The prioritization order differs:
| Intervention | Effect on Visceral Fat | Effect on Subcutaneous Fat |
|---|---|---|
| Caloric deficit | Strong — visceral fat mobilizes relatively quickly in a deficit | Strong — primary driver of subcutaneous fat loss |
| Resistance training | Strong — even without weight loss, resistance training reduces visceral fat in research populations | Moderate — preserves muscle during a cut; supports deficit adherence |
| Aerobic exercise | Strong — aerobic activity is particularly effective at reducing visceral fat per hour of effort | Moderate — contributes to overall energy expenditure |
| Sleep optimization | Strong — sleep deprivation specifically increases visceral fat accumulation | Moderate — poor sleep disrupts hunger hormones |
| Stress reduction | Strong — chronic cortisol elevation specifically drives visceral fat accumulation | Moderate — cortisol also increases overall fat storage |
Visceral fat responds faster to intervention than subcutaneous fat in most research, particularly with aerobic exercise. This means you may be making significant metabolic progress before your mirror or your photos show visible change. The absence of visible results in the first 2–4 weeks does not mean the protocol isn't working — it may mean you're burning the fat that matters most first.
Tracking the Fat You Can See
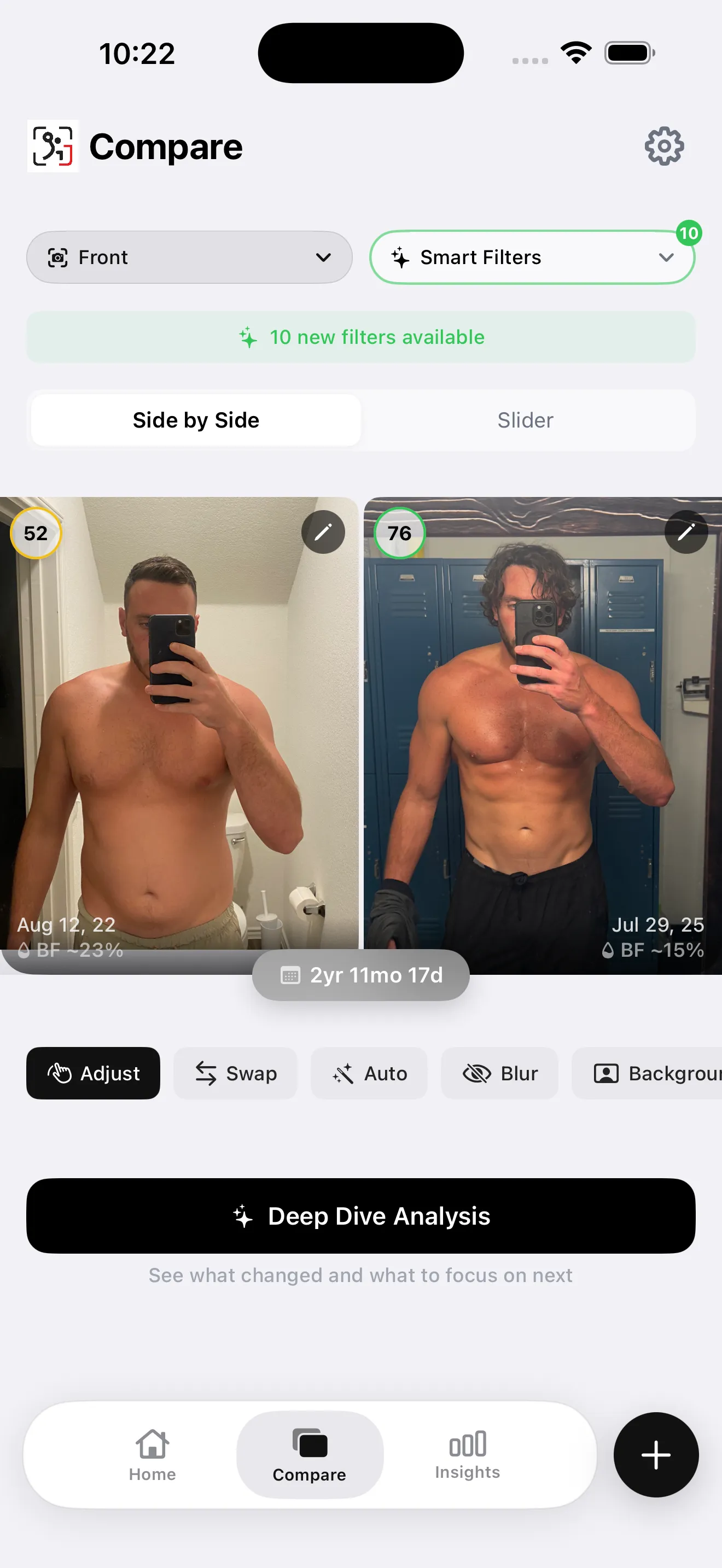
Progress photos are the most sensitive tool available for tracking subcutaneous fat changes over time — more sensitive than a scale, which conflates fat loss with muscle gain and water shifts. A side-by-side comparison taken under consistent conditions (same time of day, same pose, similar lighting) captures subcutaneous changes that the scale can't distinguish and that BMI is blind to entirely.
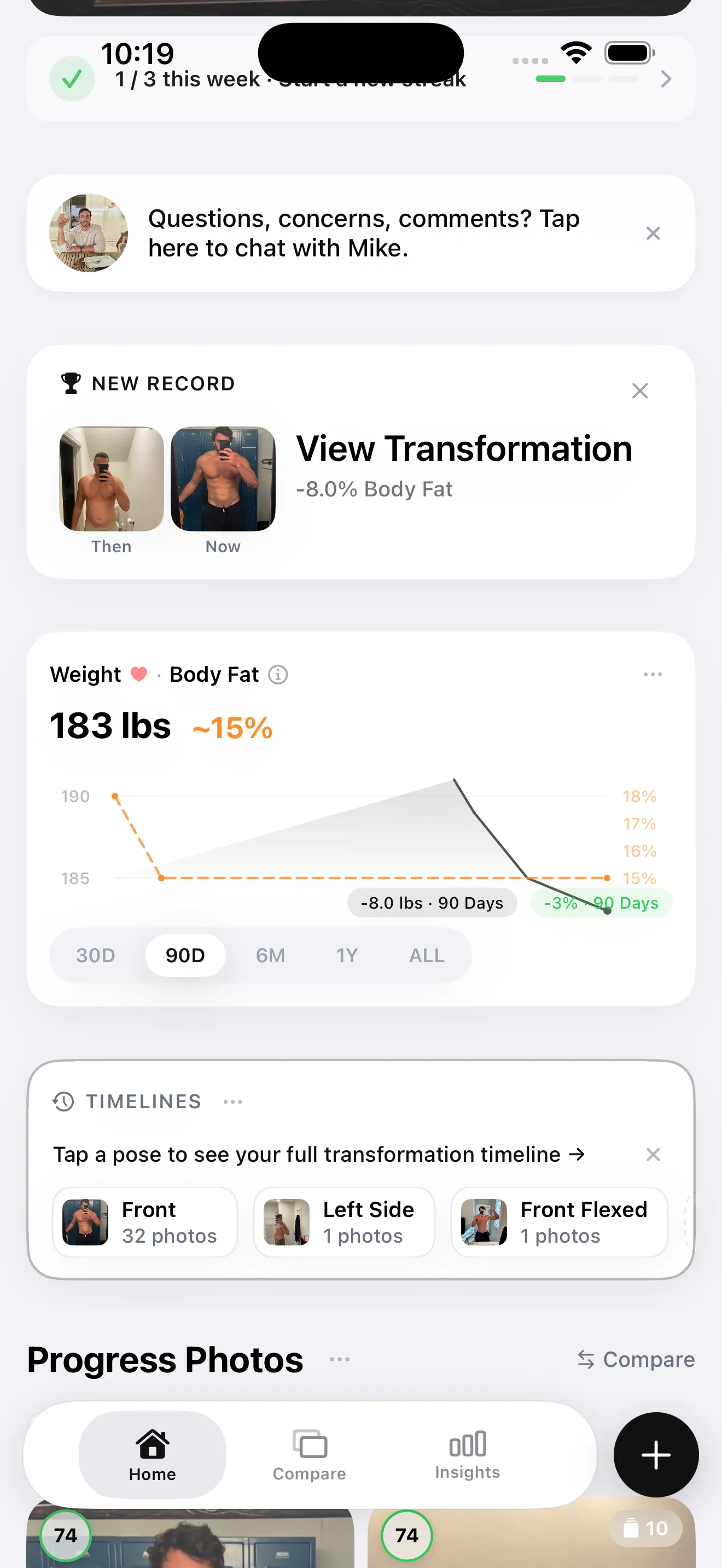
GainFrame tracks body fat percentage trend across check-ins — giving you the data layer behind the visual. A falling body fat percentage trend alongside stable or improving photos is the confirmation that the caloric deficit is working. For visceral fat specifically, the signal is indirect: sustained body fat reduction over weeks is the most reliable indicator that visceral fat is also being addressed, even though no photo will show it directly.
A Simple Framework for Tracking Both Types
- Measure your waist circumference monthly. This is your best low-cost proxy for visceral fat burden. Track the number over time; a shrinking waist circumference is strong evidence that visceral fat is reducing alongside subcutaneous fat, even if photos don't look dramatically different yet.
- Use progress photos for subcutaneous tracking, not visceral. Photos are excellent at capturing the fat you can see. Don't interpret the absence of visible change as evidence that nothing is happening internally — especially in the first 4–6 weeks of a new protocol.
- Prioritize resistance training and sleep alongside your caloric deficit. Both have specific, research-supported effects on visceral fat reduction beyond what caloric deficit alone achieves. Resistance training preserves muscle while the deficit burns fat; sleep deprivation specifically worsens visceral fat accumulation.
- Reassess every 6–8 weeks. Subcutaneous fat changes become visible over this timeframe in most people in a meaningful deficit. Waist circumference often shows measurable change earlier than the mirror does.