The bodybuilder's GLP-1 question
You already lift. You already track macros. You've cut before — probably more than once. You know what 16 weeks of low-grade hunger feels like, and you know the willpower drain that compounds in weeks 10 through 16 when the deficit is dragging on every decision you make. Then a friend at the gym mentions semaglutide. The hunger goes away. The cut keeps going. The math you've been running in your head for years suddenly stops fighting you.
That's not a hypothetical anymore. It's a real, growing pattern in the lifting community: GLP-1s used off-label, under doctor supervision, as a cutting tool. The medical search results for this question are nearly all "don't do this" — safety warnings, lawsuit ads, talking-head endorsements. None of them answer the question lifters are actually asking, which is: if I'm doing this, how do I do it without losing what I built?
This article isn't about whether to use a GLP-1. That's a conversation between you and your prescriber. This is about the protocol and the tracking — what to do once the prescription is in your hand, so the cut comes out the way you wanted it to.
The muscle-loss problem in numbers
The reason this question matters is that the default outcome on a GLP-1 is bad for a lifter. The clinical research on semaglutide (Ozempic and Wegovy) consistently shows the same composition pattern: without protective interventions, roughly 60% of weight lost is fat and 39% is muscle. That's the headline number across the major trials. Tirzepatide (Mounjaro and Zepbound) is meaningfully better — closer to 75% fat / 25% muscle in clinical work, partly because the GIP component appears to spare lean tissue better than pure GLP-1 agonism. Either way, you are not on a normal cut. You are on a cut where the body is being told to stop eating in a way that bypasses normal hunger signaling, and the metabolic shortcut comes with a tax.
The math is the part that should get a lifter's attention. A 30-pound drop on the default trajectory:
- Semaglutide, no intervention — 18.3 lb fat, 11.7 lb muscle. That's the difference between a heavy squat day and a deload week, sitting on your frame, gone.
- Tirzepatide, no intervention — 22.5 lb fat, 7.5 lb muscle. Better, but still real.
- Either drug, with the protocol below — 22.5 to 25.5 lb fat, 4.5 to 7.5 lb muscle. That's the range a normal hard cut produces, with a lifter who knows what they're doing.
Eleven and a half pounds of muscle on a 200-pound lifter is roughly 6% of total mass. That's the difference between "looks shredded" and "looks deflated." It's the difference between hitting your old bench top set in the new mirror and watching the bar feel heavier on the way back up. The whole reason a lifter cuts is to keep the muscle and lose the fat. The default GLP-1 outcome inverts the goal more than most people realize until they see it on themselves.
The good news in those numbers is the third bullet. The protocol works. The cut on a GLP-1, executed properly, can come out at the same composition ratio as a clean natural cut. It just doesn't happen by accident. Below is what "executed properly" looks like in practice.
Pillar 1: Resistance training, 3-5x per week
Mechanical tension is the signal that tells your body to keep muscle through severe energy restriction. If the signal isn't there, the body has no reason to spare muscle tissue when it needs amino acids — and a 1,000-calorie deficit needs amino acids. Lifting through the cut is non-negotiable. The structure that works:
- Compound lifts as the spine of every session. Squat, deadlift, bench, overhead press, row. These movements load the most tissue with the highest stimulus-to-fatigue ratio, which matters disproportionately when recovery is constrained by the deficit. Isolation work is fine, but the compound work is what keeps you in muscle.
- Progressive overload — but realistic. In a deficit, you are not adding weight every week. The win is holding weight at the same reps, or adding a single rep at the same weight. Track the trend over a 4-week window, not session-to-session. Maintenance of strength is progress when the calories are this low.
- Volume: 10-20 hard sets per muscle group per week. The well-established hypertrophy range. Some people will need the lower end for recovery; advanced lifters can hold the higher end if sleep and protein are dialed in. Below 10 sets per muscle group per week and you're under the maintenance threshold for trained tissue.
- Intensity stays high. RPE 7 to 9 on working sets. The reflex on a GLP-1 cut is to drop intensity because energy is lower and the deficit feels heavy. Don't. Low-intensity, high-rep "pump work" is not a stimulus the body will preserve muscle for. Hard sets are.
- Don't drop training to "preserve energy." The deficit is what makes the GLP-1 work. The lifts are what make the loss come from fat. Cutting either side breaks the equation.
One practical note: log every session. Strength data is the single highest-signal indicator that your protocol is working, and you can't read the trend without the log. Hevy is the cleanest free option for this. Strong is a solid alternative if you prefer its UI. Either one. Pick one and use it every session.
Pillar 2: Protein at 1.6-2.2g per kg of body weight
The International Society of Sports Nutrition's research-backed range for cutting is 1.6 to 2.2 grams per kilogram of body weight per day. That's the literature consensus. For a 200-pound lifter, that's 145 to 200 grams of protein per day. The high end of the range is what you want when the deficit is deep and the goal is full muscle preservation — and a GLP-1 cut is a deep deficit.
Distribution matters as much as the daily total. Spread the protein across 4 to 5 meals, 25 to 40 grams per meal. That's the per-meal range that maximally stimulates muscle protein synthesis (the leucine threshold sits around 2.5g, which is roughly 25g of complete protein). One 200g protein binge at dinner does not produce the same MPS response as four 50g feedings across the day.
The hard part on a GLP-1 is not the science. It's the execution. The drug works by suppressing appetite — that's the whole mechanism — and you are now trying to force-feed yourself 200 grams of protein a day while your body is telling you it's full after 600 calories. That collision is the most underrated reason lifters lose muscle on these drugs: not the medication itself, but the failure to hit protein because hunger isn't there to drive the eating. Tactics that work for the appetite-suppressed:
- Protein shakes are not a fallback — they're the foundation. Two whey shakes per day, 40g each, gets you to 80g before any food enters the picture. The shake is liquid, fast, and goes down even when solid food sounds repulsive.
- Greek yogurt, cottage cheese, skyr. Calorie-dense, protein-dense, and easier to consume than chicken breast when appetite is gone.
- Lean meat scheduled, not chosen. If you wait until you're hungry to decide on chicken, you'll skip the meal. Schedule the protein the way you schedule the lifts.
- Protein bars for the gap meals. Quest, Built, Barebells. 20 grams in a 200-calorie package fills the math when nothing else sounds good.
- Track macros with MacroFactor or a similar app. "I think I hit my protein" doesn't survive contact with appetite suppression. The number on the screen does.
If you cannot hit 1.6g/kg consistently, you do not have a muscle preservation protocol. You have a weight-loss protocol with optimistic intentions. This is the pillar most lifters miss because it's invisible — the lifts feel right, the photos look fine for the first month, the protein gets miscounted, and at month 4 the strength chart finally exposes what was happening the whole time.
Pillar 3: Sleep 7-9 hours
Muscle protein synthesis is highest during sleep. Growth hormone pulses overnight. Testosterone in trained men correlates strongly with sleep duration. Cutting calories already pulls on these systems; cutting sleep on top of cutting calories is the fastest way to send a recovery-limited body into catabolism. There is no protein target high enough to compensate for chronic 5-hour nights when a GLP-1 is also pulling on the system.
One specific GLP-1 issue worth flagging: many users report disrupted sleep, especially in the first few weeks after a dose escalation. Some of that is the drug. Some of it is timing. Many lifters do better dosing in the morning rather than at night — the peak GI effects coincide with waking hours instead of falling on top of the sleep window. If your sleep has degraded since starting the medication, the dosing time is the first variable to test.
Practical hygiene: same bed time, same wake time, dark room, no screens in the last 30 minutes. Standard sleep advice that nobody follows until they realize how much it costs. On a GLP-1 cut, the cost is muscle. Apple Health tracks sleep duration and consistency for free if you wear a watch — the data is there if you want to read it.
Pillar 4: Slow titration
This is the pillar most under your control and most often misused. The escalation schedule on every GLP-1 is a ladder — semaglutide steps up roughly monthly from 0.25mg to 2.4mg, tirzepatide from 2.5mg to 15mg. The default assumption is that more is better and faster is better. For a lifter, that assumption is wrong.
The body can only mobilize so much fat per week. The literature on natural cutting puts the upper limit on healthy fat loss at roughly 1% of bodyweight per week — call it 1.5 to 2 pounds for a 200-pound lifter. Anything above that, the loss has to come from somewhere. The "somewhere" is muscle, glycogen, and water. On peak GLP-1 doses, weekly losses of 2 to 3% of bodyweight are reported regularly. That rate is incompatible with muscle preservation, full stop.
The lifter's titration target:
- Aim for 0.5 to 1.0% of bodyweight per week. 1 to 2 pounds for a 200-pound lifter, week over week, on the trend (not any single weigh-in).
- If your weekly rate exceeds 1.5%, you are dropping too fast. The protocol response is to either hold the current dose instead of escalating, or step the dose back down. Talk to your prescriber — most are willing to slow the ladder if you ask.
- Eat enough to land in that window. The deficit on these drugs is automatic from appetite suppression. The fix when loss is too fast isn't usually "lower the dose" first — it's "eat more food at the current dose." 300 extra calories of protein and carbs per day will frequently bring the rate down without changing the medication.
The motto for this pillar: faster weight loss is not better weight loss. It's just faster muscle loss. The whole point of using a GLP-1 as a cutting tool is to extend the deficit comfortably, not to accelerate it past the muscle-preservation envelope.
How to track if it's actually working: the tripod
Three data points, sampled at 2 to 3 week intervals, will tell you whether the protocol is working. Together they form a tripod — any two of them can lie, all three together can't. Skipping any leg of it leaves you guessing. With it, you'll know within three checkpoints whether your cut is on the rails.
Leg 1: Strength
Strength on compound lifts has the highest known correlation to muscle mass in trained lifters. If the bench is holding, the bench muscle is holding. If the squat is dropping out of proportion to the deficit, the squat muscle is dropping. The signal is unusually clean — much cleaner than circumference, body fat estimates, or how-you-look-in-the-mirror.
What to track:
- Top sets on the main compound lifts, every session, in Hevy or Strong. Squat, deadlift, bench, OHP, row.
- Specific watch-outs. Lateral raises (rear and side delts atrophy fast on a deep cut). Tricep pushdowns (the long head goes first — pushdown weight dropping is an early signal). Calf raises (often forgotten, often the first to lose mass).
- The threshold. If any compound lift loses more than 10% of its top working weight over 4 weeks, the cut is too aggressive. The protocol response: more protein, more food, slower titration.
The strength data is also where the deficit's emotional cost gets clarified. Lifts feeling heavier than usual is normal in any cut. Lifts being heavier and the bar going up slower and the top set dropping is the muscle-loss signature.
Leg 2: Body composition — BF%, lean mass, FFMI
Strength alone can hold for a while even when muscle is starting to bleed (the nervous system is good at masking the first 5% of loss). Body composition catches what strength misses. The options:
- DEXA quarterly. Gold standard. $100 to $150 per scan. Catches the truth, but the cadence is too slow to drive weekly decisions — you find out about the muscle loss after 12 weeks have already passed.
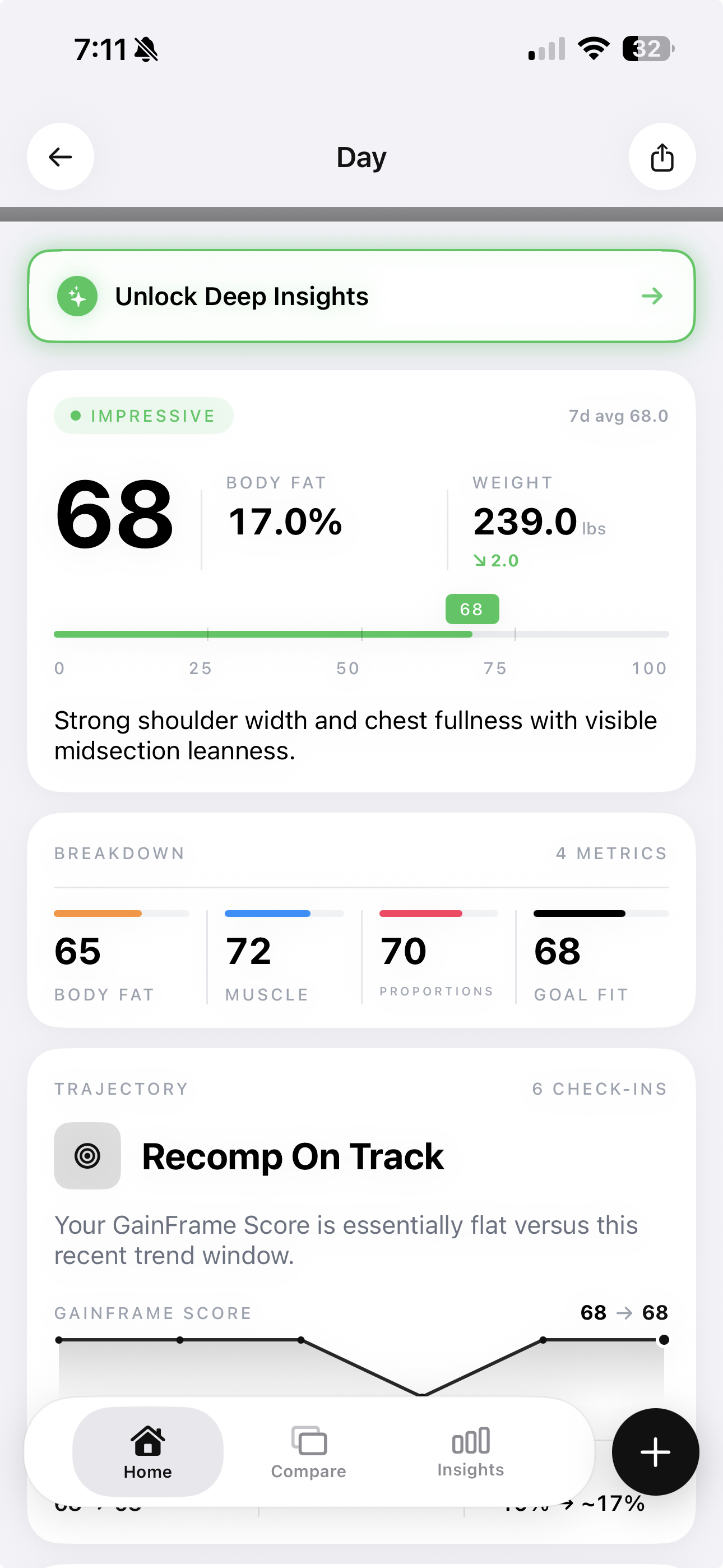
- Home AI body composition. GainFrame, Spren, trackBod. Photo-based, weekly cadence, free or low subscription. The accuracy is not DEXA, but the trend over 4 to 8 weeks is reliable enough to drive protocol changes — and the cadence is what matters when you need to catch a problem in time to fix it.
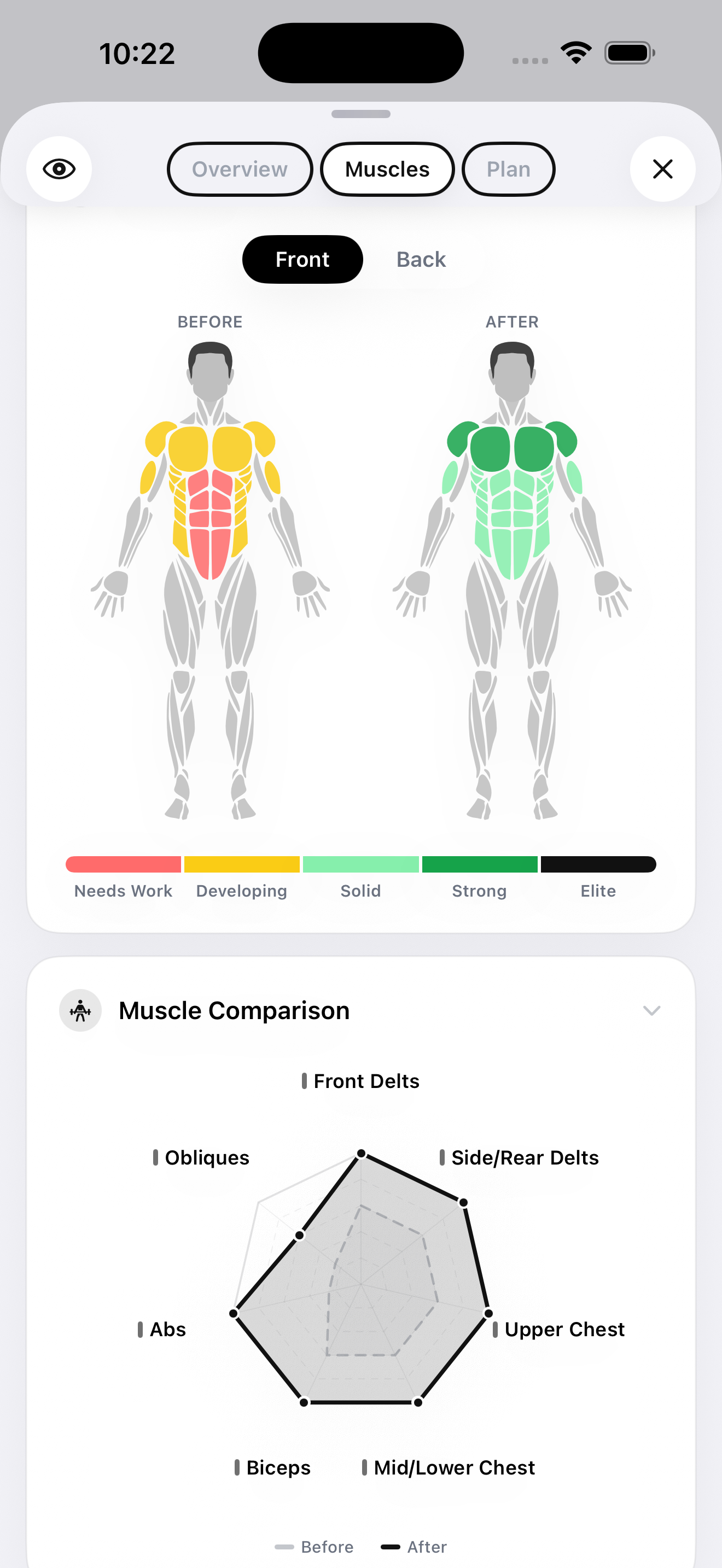
The 12-muscle-group breakdown matters more on a GLP-1 cut than on a normal cut. Whole-body BF% can hold steady while a specific muscle group is bleeding — rear delts and triceps are the usual suspects, because they're small, slow to recover, and don't get prioritized in most training programs. A per-muscle-group view catches asymmetric atrophy before it becomes a strength regression. That's the gap GainFrame's muscle map exists to fill.
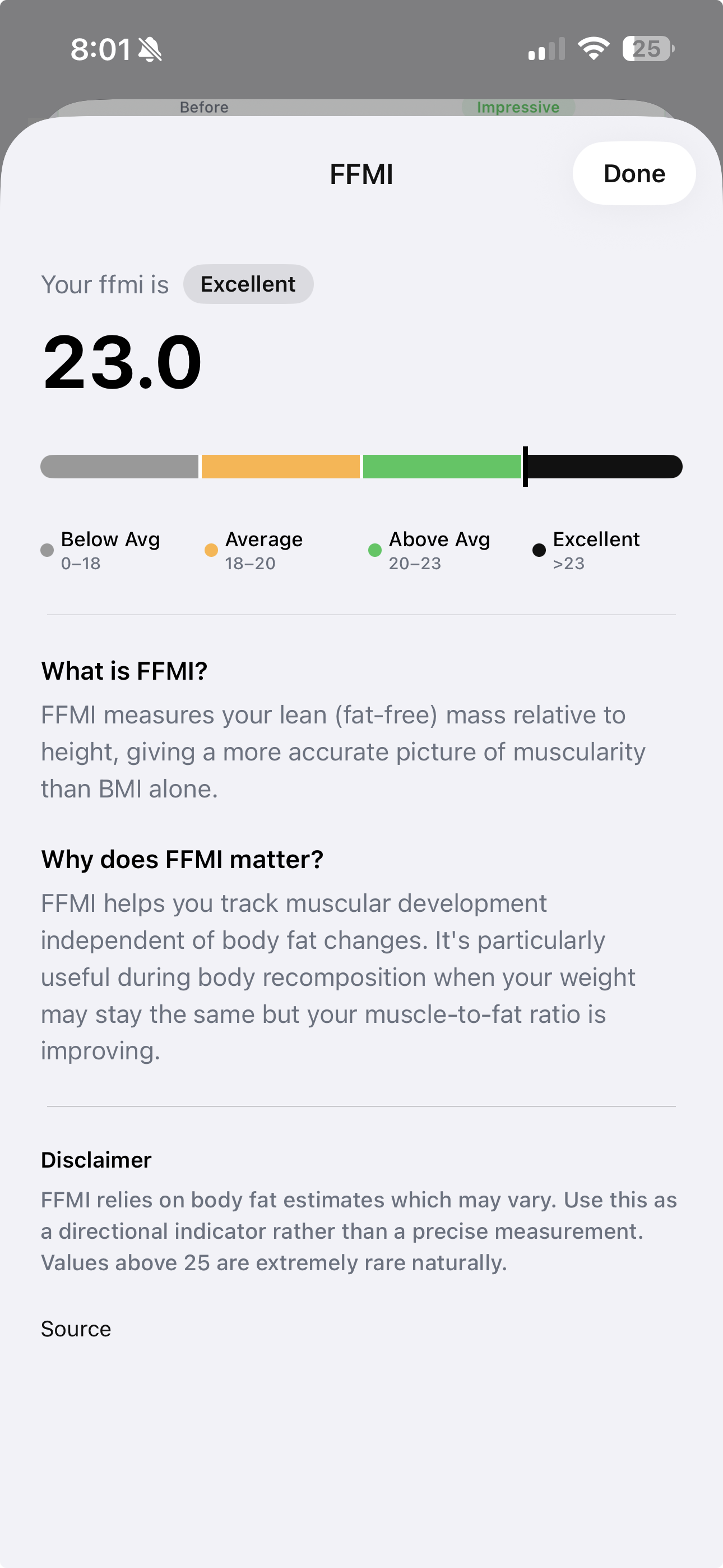
Of all the body composition metrics, FFMI is the cleanest single signal. It normalizes lean mass to height, which means it doesn't drift the way body fat percentage does when total mass is dropping. On a successful cut, FFMI should hold steady or rise slightly while body fat drops. If FFMI is falling alongside body fat, the cut is taking lean tissue. That's the canary metric — it goes off before strength does, before the photo shows it, before the lift log catches it.
Leg 3: Visual proof — photos
Photos are the third leg because the eye still catches things the data misses — posture changes, distribution shifts, the quality of the muscle that data can't quite quantify. Weekly photos, same conditions, three angles plus one flexed.
The full setup is in how often you should take progress photos and ozempic before-and-after photos — the GLP-1 specific addition is the flexed front shot. Relaxed photos look great when fat loss is happening; they hide muscle loss. Flexed photos expose whether the muscle volume is actually still there underneath.
What to watch in the photos specifically:
- The cap of the deltoid. The round shape disappears first when shoulder muscle drops.
- The tricep horseshoe. Visible from the side and back when arms are hanging. Flat triceps are a leading indicator of arm muscle loss.
- Lat width. The taper from shoulder to waist tells you whether the back is holding mass while the waist drops.
Take both flexed and relaxed shots every session. Relaxed shows fat-loss progress — the fun half of the story. Flexed shows muscle preservation — the half you actually need to see.
Warning signs you're losing too much muscle
The protocol works on average. It doesn't work universally — individual recovery, training history, sleep, stress, and dose response all vary. The point of the tracking tripod is to catch the cases where it isn't working in time to do something about it. The signals that matter:
- Strength dropping faster than expected. Greater than 10% loss in any compound lift over a 4-week window. That's beyond what a normal deficit would do.
- Bench or OHP feeling like dead weight at usual reps. Subjective, but consistent across sessions. The bar shouldn't feel categorically heavier — it should feel like the same weight on a tired day.
- Lateral raises impossible at usual weight. Lateral raises are tiny isolation movements; the absolute weight is so small that fatigue alone shouldn't change the number much. When it does, it's near-pure muscle loss.
- "Flat" appearance despite weight loss. Muscle volume is gone, not just fat. The mirror reads "smaller" instead of "leaner." The flexed photo no longer pops the way it used to.
- FFMI dropping. The cleanest single signal. If FFMI is falling on the same week-over-week curve as body fat, you are not running a cut — you are running a weight loss protocol.
- Body fat percentage NOT dropping despite weight loss. If the scale is dropping but BF% is holding flat, you're losing muscle and fat in roughly the same proportion. That's the worst possible outcome and the easiest to miss because the scale is "going down."
When two or more of these show up at the same time, the cut is off the rails and the right move is to slow it. The order of operations: increase calories first (300 to 500 per day, mostly from protein and carbs), hold the dose instead of escalating, and if the signs persist into the next checkpoint, step the dose down or pause entirely. The cut is supposed to make you smaller AND leaner. If it's only making you smaller, it's not a cut anymore.
The honest verdict
You can preserve most of your muscle on a GLP-1 cut. The data supports it, the protocol exists, and lifters who execute it cleanly come out the other side at composition ratios that look like a normal hard cut. But it's not automatic. Without resistance training, deliberate protein, sleep, and slow titration, the math runs against you and the default 60/39 outcome is what shows up in the mirror at month 6.
The tracking is what makes the protocol credible. Without weekly strength logs, monthly body composition data, and consistent photos, you are guessing. With all three, you'll know within three checkpoints — about 6 to 8 weeks — whether your cut is producing the body composition you want or eating the muscle you spent years building.
This isn't medical advice. The medication is a conversation with your doctor. The protocol and tracking workflow above are for lifters who are already on a GLP-1 under medical supervision and want to preserve what they've built in the gym. The four pillars are research-backed, the tripod is observable in your own data within weeks, and the difference between "looks shredded" and "looks deflated" comes out of executing both — not picking one.
Track Your GLP-1 Cut the Way a Lifter Should
GainFrame tracks BF%, lean mass, FFMI, and individual scores for 12 muscle groups from your progress photos — the only home tool that catches asymmetric muscle loss before it shows up in your lifts. Pair with Hevy for the strength side, MacroFactor for protein, and Apple Health for weight trend, and you have the full muscle-preservation stack at home.
Download GainFrame Free